Kenya has made remarkable strides towards reaching the UNAIDS 95-95-95 HIV targets for epidemic control, and HIV and tuberculosis (TB) services now reach a significant proportion of the Kenyan population.
According to the Kenya Population-based HIV Impact Assessment (KENPHIA), 79.5% of adults who tested positive for HIV were aware of their status prior to the survey, 96% were on antiretroviral therapy (ART), and 90.6% had achieved viral load suppression. Maintaining this progress requires concerted efforts between the government and its partners to ensure the sustainability of successful interventions, as well as the exploration of new evidence-based public health strategies informed by evaluations, surveillance, and research.
In 2016, the University of Maryland, Baltimore (UMB) through Ciheb partnered with the Centers for Disease Control and Prevention (CDC) to implement a new five-year program called “Technical Assistance for Public Health Impact in Kenya” (TAPHIK).
TAPHIK’s main purpose was to provide technical and programmatic support to the Kenya Medical Research Institute (KEMRI). Specific objectives included supporting laboratory testing, surveillance, and investigations on infectious diseases.
In year four (October 2019 to October 2020) of its implementation, TAPHIK reached a number of milestones, including performing 5,081 tuberculosis tests. As of January 2021, the program also conducted 147 laboratory multi-drug resistant TB (MDRTB) surveillance tests.
TAPHIK also included multiple studies and surveillance systems that Ciheb implemented or supported KEMRI to implement in Western Kenya, including:
These studies and surveillance systems from the KEMRI-TAPHIK collaboration helped fill a need for HIV research in Western Kenya and Kenya in general.
“The public health evaluation, or the public health agenda, is broad,” explained Dr. Emily Koech, CEO of Ciheb-Kenya. “We saw TAPHIK as an opportunity for Ciheb to be involved in that aspect of asking the questions, not just in Western Kenya, but countrywide.”
Surveillance systems are critical in HIV programming as they help with identifying locations and populations most affected, adapting delivery of HIV services for maximum efficacy and efficiency, and monitoring progress.
The HDSS platform was created decades ago and is a foundation for many epidemiological studies and evaluations of public health work in Kenya. HDSS contains population-based demographic data of about 220,000 people within Siaya County and is periodically updated with new data from the field.
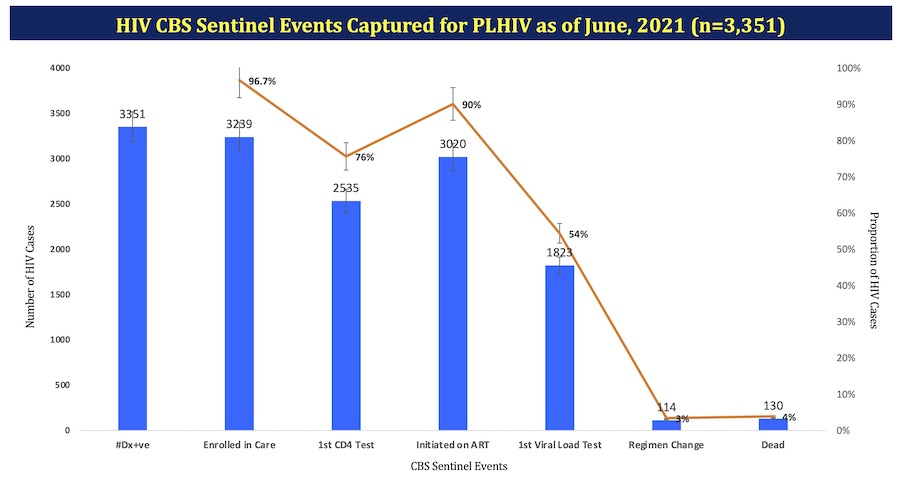
In 2020, Kenya released guidelines on CBS to monitor key indicators along the HIV treatment cascade. TAPHIK piloted CBS in 14 facilities in Gem Sub-county in Siaya County and developed a system linking facility electronic medical records with information in the HDSS platform in order to monitor sentinel events and outcomes for HIV-infected clients.
CBS for electronic medical records has now been rolled out nationally through a phased approach with select counties. In 2021, TAPHIK implemented Kenya’s first ever HIV paper-based CBS in 30 facilities in Migori County for non-EMR facilities and is working with CDC and NASCOP to adapt this initiative nationally.
In addition to developing surveillance systems, TAPHIK conducted two surveys to collect and better understand risk factors for HIV.
The integrated biological behaviors survey (IBBS) was led by KEMRI, a state corporation charged with conducting human health research. Completed in 2018, this survey focused on monitoring fisher folk, a population that primarily resides in Migori, Siaya, Kisumu, and Homa Bay Counties around Lake Victoria and is particularly at risk of HIV infection. IBBS’ purpose was to collect behavioral and biomarker data for these communities to understand the prevalence and distribution of HIV and the behavioral risk factors.
Map showing Migori County in Western Kenya, with neighboring Homa Bay, Siaya, and Kisumu Counties.
“Sample households spread over eight islands were mapped out with face-to-face interviews conducted to collect data that included patient characteristics, HIV risk behavior, care and treatment history, with blood samples collected for rapid HIV testing,” said Constancia Awiti, the TAPHIK program manager.
Nearly 1,100 households and almost 3,800 people were sampled for this survey. Roughly 60% were adults and 40% were children, and 55% of the survey population was female. The study found fisher folk have a high burden of HIV, with risky sexual behaviors prevalent with transactional sex. IBBS found low rates of condom use with casual partners, with almost two-thirds (63%) of participants reporting not using a condom during their last sexual encounter, which was persistent with known risk. ART coverage was high (96%), but knowledge of HIV-positive status was moderate (80%).
The second TAPHIK supported survey was the longitudinal biobehavioral survey (LBSS), which was conducted to determine the trends in behavioral risk factors, incidence, and prevalence of HIV among people older than 13 years enrolled in the HDSS platform, and to evaluate the level of coverage of HIV interventions in Gem Sub-county within Siaya County.
Out of 16,140 enrolled individuals, 97% completed the survey, 60% were female, and the median age was 31 years. A total of 14,208 participants were eligible for screening, out of which 81.3% were tested. Nearly 25% of girls 13-14 years of age reported having ever had sex. The median age of sexual debut was 16 and similar among males and females. The 2018 survey indicated that the HIV program in Gem Sub-county achieved all three UNAIDS 90-90-90 targets overall, and for both women and men.
As the program comes to a close, Ciheb is working to ensure that the achievements from the last five years can be sustained by KEMRI.
TAPHIK, along with KEMRI and other partners, have been able to monitor affected locations, collect data, train staff, and strengthen public health facilities and systems. All of this helps to guide Western Kenya, and Kenya as a whole, on a path to reducing the transmission of HIV and improving HIV outcomes eventually achieving the 95-95-95 targets.