HIV care and treatment involves complex needs and a unique set of circumstances for each client, and the conventional one-size-fits-all approach to treatment does not best serve people living with HIV (PLHIV). The client-centered approach known as differentiated service delivery (DSD) provides creative solutions to tailor clinical services to meet the needs of each client, an approach that better serves clients and the Kenyan health system.
Ciheb in Kenya, through the PACT Timiza program that recently completed in the Western Kenyan counties of Kisii and Migori, used DSD to support an estimated 90,000 PLHIV with a variety of health services.
DSD provides myriad benefits, such as refocusing resources to those most in need or requiring fewer clinic visits for individual patients.
“Clients who are HIV positive don’t come to the hospital very sick in poor health,” said Dr. Angela Ndaga, senior technical advisor for PACT Timiza. “Their management of HIV is similar to having any other chronic illness, such as hypertension or diabetes. The healthcare provider is able to walk with this client through their journey towards better health outcomes, which results in a healthy client who is healthy enough to go about their day-to-day work.”
PACT Timiza started implementing DSD in 2017 following the national launch of the Differentiated Care Operational Guide 2017. The program had packages of care based on initial and follow-up evaluations to categorize a PLHIV as either well/advanced or stable/unstable. The categorization was based on age, clinical, virological, and psychosocial assessments.
Within a stable population, the program had either facility-based or community-based service delivery models. The unstable population included children, adolescents, and pregnant women seeking services within the maternal and child health clinic, PLHIV with advanced disease (WHO Stage III and/or CD4 <200), and viremia patients (viral load copies of >1000 copies/mL).
When clients visited a facility, they were met by a peer navigator or educator. The client was then triaged and categorized as either stable or unstable. In June 2021, PACT Timiza was supporting 92,216 people, and more than 90% (83,545) were PLHIV who had been on ART for more than a year. Of that PLHIV population, 79% were considered stable, of whom 91% were placed on a differentiated care model.
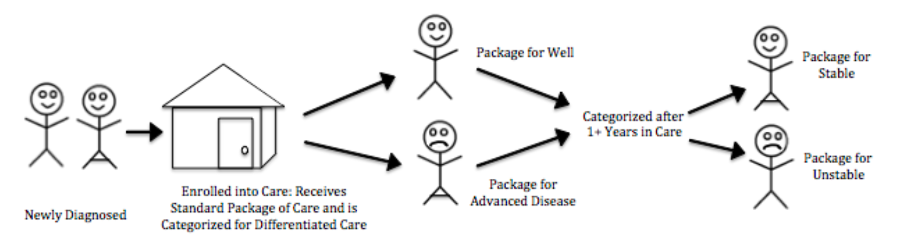
Differentiated care based on patient clinical status
Multi-month dispensing (MMD), in which a client is sent home with three- or four-months’ worth of medication, was another facet of DSD. MMD for stable clients provided several advantages, such as reducing the time spent at the facility, the number of clinic visits, and medical costs. The client would see the clinician in follow-up visits at least twice a year if there were no acute issues.
Within Kisii and Migori Counties, PACT Timiza implemented different clinics for different demographics. These included men-only clinics, Operation Triple Zero (OTZ) and OTZ Plus clubs (“Plus” meaning HIV-positive pregnant or breastfeeding adolescent girls), and Papa Mama (PAMA) clinics. The men-only clinics track male-related issues like alcoholism and gender-based violence and organized discussion groups to address them. One example is the support group for men who abuse alcohol in Isecha, Kisii County. The group enrolled men recovering from alcoholism with high viral load and served as an alcoholics anonymous-type group that had representatives pick drugs for members from the facility.

Lilian Okioga, a peer navigator/educator supported by PACT Timiza, inspects a box of medication
“We’re able to engage the men during the family clinics where we have a whole household coming into the facility,” said Dr. Ndaga.
Within the OTZ clubs, the program focused on HIV care in line with the triple zeros: zero missed appointments, zero missed drugs, and zero viral load. For those who were in the maternal and child health clinic — the OTZ Plus clubs — PACT Timiza focused on zero HIV transmission to the unborn child. PAMA clinics were a family-centered DSD model which focused on the well-being of the child as well as that of the mother, father, or any caregiver that supports the child within the HIV clinic.
Providing DSD requires a level of flexibility by the healthcare system. Due to issues of stigma, there were challenges with operating community ART groups (CAGs) with only 601 CAGs and 5,521 PLHIV (9% of those on a DSD model) enrolled. CAGs tended to appeal more to rural rather than urban residents. Other clients were more comfortable in group meetings at the clinical facility, known as facility ART distribution groups (FADGs), as opposed to group meetings with neighbors.
DSD also addressed the different needs in urban versus rural settings. Urban clients mostly preferred the fast-track model, where clients were in and out of an express clinic in 10 minutes and some clinics opened as early as 6:00 a.m. This was less suitable to a rural setting, where the lifestyle is slower and organizing facility or community groups is more feasible.
“If a client prefers an express model of ART distribution, then that is what the client will receive,” Dr. Ndaga said. “At the end of the day, it’s focusing on the client’s need and not the healthcare worker’s need.”
PACT Timiza worked well with the respective county and sub-county health management teams. During mentorship and technical assistance sessions at facilities, program staff worked alongside county and sub-county teams.
“We conduct joint mentorship with the county and sub-county mentors,” Dr. Ndaga said.
This shared experience and the standard operating procedures that have been implemented will ensure the continuity of care for the more than 90,000 PLHIV in Kisii and Migori Counties as the government health management teams take the lead from PACT Timiza.